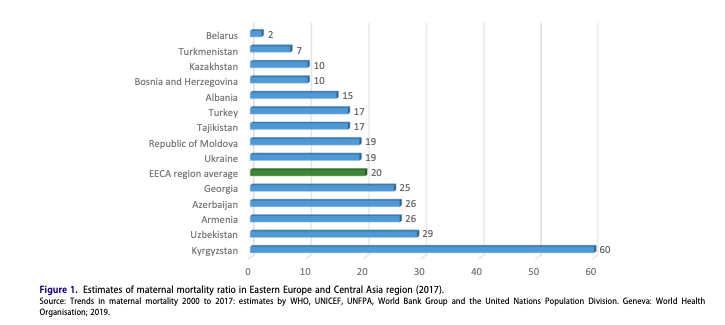
For women who migrate, access to health care, in general, is extremely restrictive. However, reproductive health care has become an even more restrictive resource, especially for women who do not have citizenship or legal status in the country they reside in. Migrant women, compared to men, face increasingly more challenges due to restrictive medical barriers as well as sexual assault, which could more likely lead to unwanted pregnancy and sexually transmitted diseases (Mahmood, 88). Interestingly, while reproductive healthcare can often be restrictive, there is data to support the idea that migrant women do often obtain abortion services abroad, regardless of citizen status. However, many of these women obtain abortions in unsafe and unsanitary places. These unregulated abortion services for migrant women lead to high rates of maternal mortality. In the above graph, we can see how, compared to many Eastern European nations, women obtaining abortions in Central Asia have a way higher MMR (maternal mortality rate), with Kyrgyzstan having the highest. Often times, countries with high MMR occur when preventable situations, such as sepsis, anemia, and eclampsia, could have been avoided. The need for regulated abortion services for migrant women are clear, but many migrant-receiving governments refuse to fund these resources, which is ironic given that many of these governments are xenophobic and do not want a permanent immigrant population.
There is a huge lack of sex education, anti-sexual violence legislature to protect survivors, and reproductive healthcare and family planning services. Governments who advertise female migration, especially for work in domestic and eldercare sectors, need to recognize that the intersectionality of women migrants means that there is a different criteria to be met. For example, if female migrants are needed in Italy for elderly care, that there needs to be an acknowledgment from the Italian government that female migrants have different experiences than male migrants, and therefore require different compensation. This should include access to all the SAME health resources that Italian women do, such as family planning, contraceptives, sex education, etcetera. While there will certainly still be language barriers to make it more difficult for some migrant women to access these resources, this will demonstrate the government’s attempt at providing a more welcoming acceptance of female migrants into Italy. An example of a government publicizing their reproductive health services for women migrants successfully can be seen in Sweden. In Gothenburg, Sweden’s second-largest city, 40% of its residents are foreign-born and speak over 40 different languages. In order to address the language barrier, the government trained women of different backgrounds to be reproductive health care representatives for their respective communities and could also act as translators. These health officials already have pre-existing bonds with the women of their community and could communicate effectively with them to increase the migrant women’s access to these resources (Smith, 23).
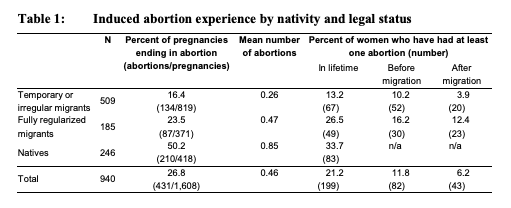
Over the past 25 years, contraception in Eastern Europe and Central Asia has increased steadily over the past 25 years (Mahmood). In another article that compared abortion in Russia among natives and migrants, the author found that there were higher rates of induced abortion among native Russian women (Agadjanian). In addition, permanent migrants, compared to temporary migrants, had way higher rates of abortion. Another aspect I found interesting was that temporary migrants had way higher rates of using long-term contraception (28%) compared with only 0.8% of Russians using this form of contraception. This could be attributed to the fact that migrant women cannot afford to get pregnant due to lack of abortion services, and long-term contraceptives are safer than short-term such as condoms and birth control pills. The authors attributed this stark difference between permanent and temporary/irregular migrants was due to the permanent migrants’ assimilation to Russia’s “abortion culture” and their greater access to state-run services (Agadjanian, 1292).
Russia, in general, has had its fair share of problems with properly providing women with these health rights. The UN has consistently called Russia out for its lack of provisions to provide women with these rights, which has a lot to do with Russia’s obsession with the declining birth rate and their deeply-rooted patriarchal culture. They have had trouble with providing not only affordable health services for women, but also have had issues with promoting sex education to adolescents, especially for women in rural areas (Center for Reproductive Rights). There has also recently been a surge of Russian Orthodox Christian activists who are actively trying to dismantle the current system in which women can have an abortion up to 12 weeks without a medical reason to obtain one (Erofeeva). The government and these activists have begun to reintroduce the “normative need” for women to reproduce, which is due to the state’s rising fears of an alarmingly high median age in the near future if birth rates continue to fall. Given this information, it is understandable why it is so difficult for migrant women to access these resources, especially those who are temporary migrants.
There was nowhere in the article that addressed issue of linguistic, financial, or societal challenges in detail. It would be interesting to see a country such as Russia mimic a similar tactic as Sweden’s where they train women of different backgrounds to be reproductive health advocates for their communities. Even if these resources become more accessible for temporary migrants, it will not be very successful if the women do not know what is available to them in the first place if there are linguistic barriers.
Bibliography
Agadjanian, Victor, and Sam Hyun Yoo. “Migration, Legality, and Fertility Regulation: Abortion and Contraception among Migrants and Natives in Russia.” Demographic Research, vol. 38, 2018, pp. 1277–1302., doi:10.4054/demres.2018.38.42.
Center for Reproductive Rights. “UN Committee Urges Russia to Fulfill Women’s Rights.” Center for Reproductive Rights, 2010, reproductiverights.org/press-room/un-committee-urges-russia-to-fulfill-women%E2%80%99s-rights.
Erofeeva, Lyubov Vladimirovna. “Traditional Christian values and women’s reproductive rights in modern Russia–is a consensus ever possible?.” American journal of public health vol. 103,11 (2013): 1931-4. doi:10.2105/AJPH.2013.301329
Smith, Alyna C, and Michele LeVoy. “THE SEXUAL AND REPRODUCTIVE HEALTH RIGHTS OF UNDOCUMENTED MIGRANTS NARROWING THE GAP BETWEEN THEIR RIGHTS AND THE REALITY IN THE EU.” Platform for International Cooperation on Undocumented Migrants, Feb. 2016, pp. 1–26.
Tahir Mahmood, Johannes Bitzer, Jacky Nizard, Mary Short & on behalf of EBCOG and ESC Issued to mark the 25th anniversary of the Cairo International Conference on Population and Development (ICPD) in Nairobi on 12th November 2019 (2020) The sexual reproductive health of women: unfinished business in the Eastern Europe and Central Asia region, The European Journal of Contraception & Reproductive Health Care, 25:2, 87-94, DOI: 10.1080/13625187.2020.1718638
You brought up some fascinating facts in this blog post that make me want to look into this subject more on my own time. I think you make some excellent points and arguments. I agree with you that countries (especially those with xenophobic tendencies towards their migrants) should want to provide reproductive/contraceptive care to their migrants. A lot of the data points you presented make logical sense. Temporary migrants showing greater use of long-term contraceptives is quite practical on their part. Most of all, I believe this to be an incredibly important issue that I imagine is often overlooked. It is also an issue that most all women can relate to and empathize with.
This is a really interesting topic, Veronica! I think you’ve done a good job capturing how many different aspects of being a migrant make it difficult to access safe reproductive care. The statistic about long-term contraception among migrants was interesting – I wonder if these women are mostly getting access to long-term contraception in Russia or elsewhere? I am also interested in that author’s use of the term “abortion culture” about Russia. What does that mean? I’ll have to check out that article!
Hi Veronica — Very interesting topic. While it seems clear that migrant women in Russia or Sweden have less access to reproductive healthcare and rights in general than Russian or Swedish women, how does their circumstance compare to women in their home countries? It seems here that the Central Asian countries have relatively low access to reproductive healthcare to begin with, so is it much of a loss to not have access to it in the countries they migrate to? Also, do you have any idea why Kyrgyzstan’s maternal mortality ratio is so much higher than every other country on that list?
There is some really new work on this topic by a recent PhD from Ohio State University, last name Zotova.
I too wonder why Kyrgyzstan’s maternal mortality rate is higher than others in the region. Uzbekistan put a big push into maternity care in the early 2000s. Tajikistan saw its maternity care sector really reformed by international organizations.
This is an interesting study. I read the comments to your post and would just like to ask everyone here to when extent lack of sex-education, access to information about women’s health in the home counties impacts the migrants ability to advocate or seek help while in Russia? I really like the recommendation based on Sweden’s approach to mobilize current female migrants as potential health-care social workers or simply dissemination of information regarding health management in their native languages because as we saw from previous films and readings Russian language skills are diminishing across former soviet countries and English has not become popular enough for it to serve as an intermediary.